CJC-F, CJC-F Announcements
Methamphetamine
Introduction
What comes to one’s mind when one thinks of methamphetamine? Perhaps the recent news of a woman, Noor Fadhilah Azlan, allowing teenagers to smoke methamphetamine in her flat – the first prosecution of an adult with drugs permitting a young person to consume drugs. Or perhaps it is the case of Ler Teck Siang, the former head of the Ministry of Health’s National Public Health Unit who was involved in the HIV data leak in Singapore and who was found to have given methamphetamine injections to patients. Perhaps it’s another case involving the drug.
Yet, those are just two of the many cases of methamphetamine abuse. Unfortunately for Singapore, there has been a growing trend in methamphetamine abuse in recent years, with the total number of methamphetamine abusers skyrocketing to over 2000 in 2018 and 2019, and the number of new methamphetamine abusers far surpassing the new abusers for all other drugs at 73% of the new drug abusers. In fact, there was a 60.9% increase in the amount of crystalline methamphetamine seized between 2018 and 2019 alone, from 19.33kg to 31.1kg.
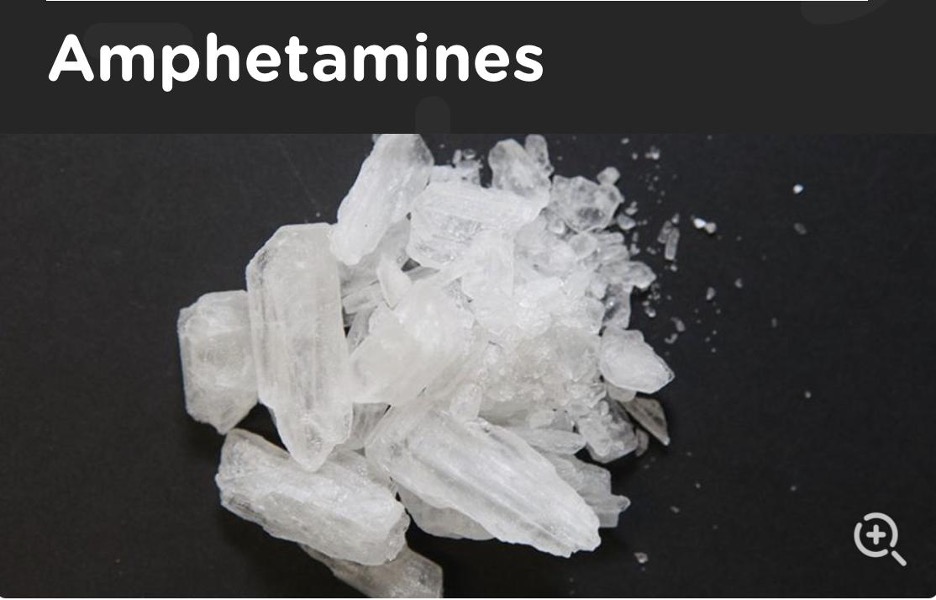
An often-encountered form of the amphetamine class.
Source: https://adf.org.au/drug-facts/amphetamines/
Methamphetamine – also known as meth, blue, ice, crystal, etc. – is a highly addictive stimulant. Like the rest of the amphetamine class, it often comes in the form of a white crystalline powder which can be taken orally, intranasally (snorting), via inhalation (smoking), or via injection into the bloodstream. Although methamphetamine is structurally similar to amphetamine, the extra methyl group attached to it results in better crossing into the brain (due to increased lipophilicity) and thus increased potency.
Legally, methamphetamine may be used in some cases of ADHD and narcolepsy. However, it is often used illegally due to its euphoric effects.
A possible reason why methamphetamine is more abused than other illicit drugs could be because of its potential to increase dopamine levels by up to 1250 times. This is five times as much as cocaine’s potential and more than eight times that of non-illicit abusable substances such as alcohol and tobacco.
Besides euphoric effects, other short-term effects of methamphetamine include increased blood pressure, wakefulness, anxiety, fast and/or irregular heart rate (arrhythmias), and decreased appetite. These effects are caused by increased dopamine, serotonin, and adrenaline in the body through inhibition of re-uptake mechanisms by methamphetamine, and increased release of serotonin and adrenaline from neurotransmitters by methamphetamine.
Longer-term effects of chronic methamphetamine use include “meth sores”, “meth mouth”, drastic weight loss, and insomnia. “Meth sores” are due to the combination of skin dryness (a side effect of methamphetamine) and the excretion of methamphetamine through sweat. The urge to pick at such sores due to the effects of methamphetamine further aggravate this. “Meth mouth” is the result of the direct acidic effects of methamphetamine, when exposed to the mouth in any form, the decreased activities of the salivary glands due to methamphetamine and decreased oral hygiene. All these lead to severe tooth decay and loss of teeth. Besides these, long-term effects include signs of rapid aging such as rapid skin aging, permanent heart and brain damage (due to the effects of constant arrhythmias and increased blood pressure), as well as kidney and liver issues in young abusers despite these conditions being associated with much older people.
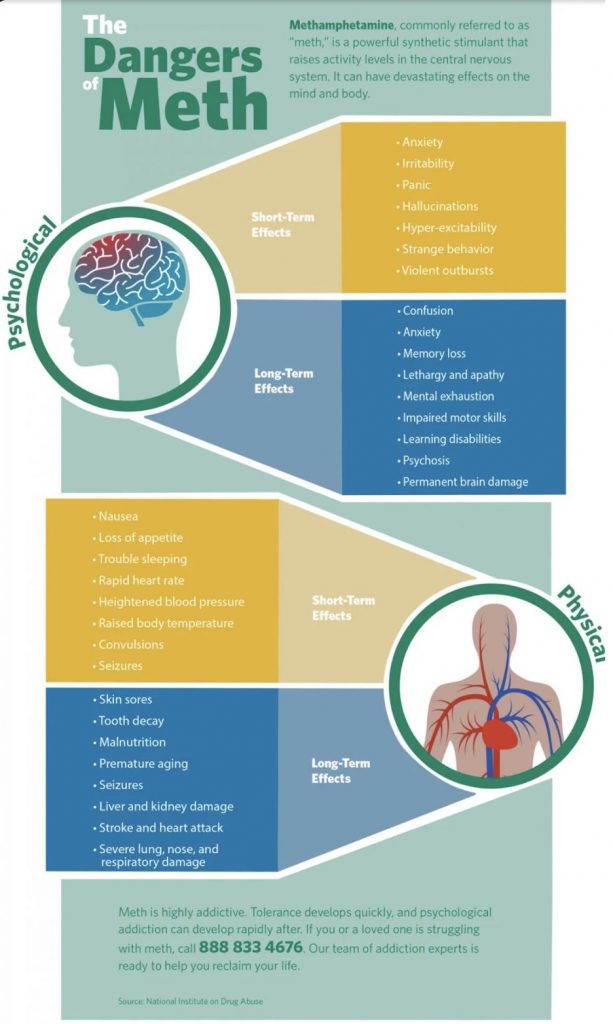
Summary of some side effects of methamphetamine.
Source: https://www.google.com/amp/s/mountainside.com/blog/drug-addiction/the-dangers-of-meth/%3famp
Where Does Methamphetamine Come From?
A common route of methamphetamine trafficking originates from Myanmar. Myanmar is the world’s biggest producer of methamphetamine. Given Singapore’s proximity to Myanmar within the region, methamphetamine trafficking definitely reaches our shores.
Unfortunately, trafficking is not the only method to obtain methamphetamine, for there exists various recipes to create it with relatively obtainable ingredients. One common way is to derive it from pseudoephedrine, a pharmacy-only medication for nasal decongestion. Though pseudoephedrine is often mixed with other medications in Singapore, and regulations on limiting pseudoephedrine sales in Singapore exist, it is unknown whether people create methamphetamine from pseudoephedrine in Singapore. (No, there will be no recipes for meth here in case anyone tries to experiment with them.)
Methamphetamine Testing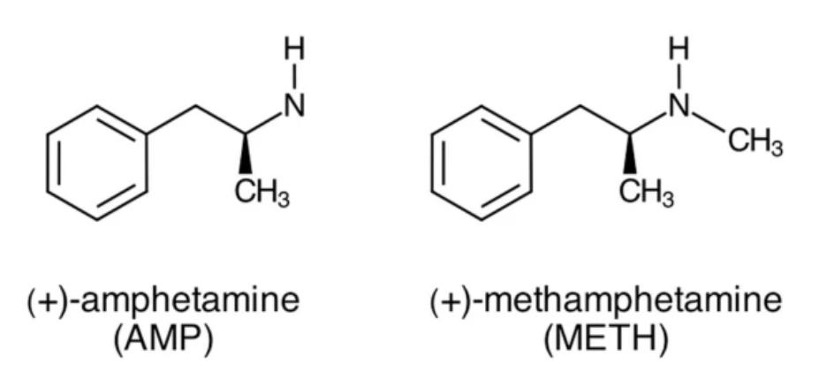
Source: https://www.nature.com/articles/srep03673
Preliminary tests can be done on methamphetamine before confirmatory tests (e.g. Gas Chromatography Mass Spectroscopy, or GCMS for short) are done. Preliminary tests include the Marquis test (for certain ring structures) and the Simon’s test (for secondary tests). Due to the lack of the certain ring structures, there would be no reactions for the Marquis test, and the mixture would remain yellowish. Meanwhile, due to the presence of a secondary amine, the Simon’s test would result in a colour change from red to blue. However, such a colour change would depend on the amount of methamphetamine tested. The Simon’s test produces different results from amphetamine as amphetamine has a primary amine (giving it negative results).
Confirmatory tests for methamphetamine are required. While the GCMS may be used to identify direct samples, confirmation of ingestion requires biological samples. As mentioned in an earlier article, methamphetamine can be detected by the presence of methamphetamine and amphetamine in blood, urine, or hair. As methamphetamine has a chiral center, it has two enantiomers- d-methamphetamine and l-methamphetamine. However, as mentioned in an earlier article, some immunoassays are unable to distinguish between d-methamphetamine (the enantiomer with euphoric and abusive properties) and l-methamphetamine (AKA levmetamfetamine, the enantiomer without stimulant effects). This poses a problem as l-methamphetamine is a metabolite of selegiline, a medication for Parkinson’s Disease and depression, and also because some nasal decongestants containing levmetamfetamine exist overseas (although the latter is an extremely unlikely scenario as levmetamfetamine is not available in Singapore). As such, caution should be taken when interpreting assays that cannot distinguish the two enantiomers.
Statutory Powers of Testing
According to Section 17 of the Misuse of Drugs Act (MDA), anyone found in the possession of more than 25 grammes of methamphetamine is presumed to have them for the purpose of trafficking, unless proven otherwise. Meanwhile, under Section 22 of the MDA, a person is presumed to have consumed an illicit drug if a controlled drug is detected in their urine (regardless of the amount) unless proven otherwise, which is a difficult burden for the defendant to discharge. Section 18 of the MDA dictates that anyone who has possession, custody, or control of keys, premises, etc. that contain the drug is presumed to have had possessed the drug and known of its nature.
As mentioned in an earlier article, Sections 31 and 31A of the MDA allow officers with at least the rank of a sergeant from the CNB, SPF, or the immigration authorities to order the production of urine and hair samples for testing if a person is suspected to have consumed an illicit drug other Section 8(b). It is an offence not to comply with such orders under sections 31(2) and 31A(2) respectively. More details can be found in earlier articles.
Conclusion
This article has summarised the worrying trends of methamphetamine usage, its reasons for abuse, mechanisms of action, and side effects. It has also noted some places the methamphetamine found in Singapore could have come from, methods for testing the presence of methamphetamine, and statutes that govern methamphetamine in Singapore.
*The views and opinions expressed in this article do not constitute legal advice and solely belong to the author and do not reflect the opinions and beliefs of the NUS Criminal Justice Club or its affiliates.
References
- 1. Lydia Lam (30 September 2020). Woman allowed teens to smoke meth in her flat, gets jail and fine in first such case. Channel News Asia. https://www.channelnewsasia.com/news/singapore/woman-allowed-teens-smoke-meth-flat-jailed-first-case-13163762
- 2. Lydia Lam (10 July 2019). Doctor in HIV data leak allegedly gave meth injections to client he met on Grindr. Channel News Asia. https://www.channelnewsasia.com/news/singapore/doctor-hiv-data-leak-meth-injections-client-grindr-sex-drugs-11708612
- 3. Rebecca Pazos and Spe Chen (1 December 2019). South-east Asia’s meth menace: one man’s struggles. The Straits Times. https://www.straitstimes.com/multimedia/graphics/2019/11/south-east-asia-meth-menace/index.html?shell
- 4. Cara Wong (6 February 2020). Number of drug abusers arrested hits six-year high. The Straits Times. https://www.straitstimes.com/singapore/courts-crime/number-of-drug-abusers-arrested-hits-six-year-high
- 5. Dominic Low (6 February 2020). 73% of drug abusers arrested in 2019 are meth users. The Straits Times. https://www.straitstimes.com/singapore/courts-crime/number-of-drug-abusers-arrested-hits-six-year-high
- 6. National Institute of Drug Abuse (October 2019). Methamphetamine Research Report: What is Methamphetamine? https://www.drugabuse.gov/publications/research-reports/methamphetamine/what-methamphetamine
- 7. Hunt D et al (2006). Methamphetamine Use: Lessons Learned, Chapter 3. NCJRS. https://www.ncjrs.gov/pdffiles1/nij/grants/209730.pdf
- 8. Anglin MD, Burke C, Perrochet B, Stamper E, Dawud-Noursi S. History of the methamphetamine problem. J Psychoactive Drugs. 2000 Apr-Jun;32(2):137-41. doi: 10.1080/02791072.2000.10400221. PMID: 10908000.
- 9. American Addiction Centres (2020). The permanent effects of drugs on the body.https://americanaddictioncenters.org/health-complications-addiction/permanent-effects
- 11. 2019, May 16. Methamphetamine DrugFacts. Retrieved from https://www.drugabuse.gov/publications/drugfacts/methamphetamine
- 12. UptoDateMethamphetamine.
- 13. Hunt D et al (2006). Methamphetamine Use: Lessons Learned. NCJRS. https://www.ncjrs.gov/pdffiles1/nij/grants/209730.pdf
- 14. Karl-Artur Kovar and Martina Laudszun (1989). Chemistry and Reaction Mechanisms of Rapid Tests for Drugs of Abuse and Precursors Chemicals. United Nations. https://www.unodc.org/pdf/scientific/SCITEC6.pdf
- 15. Singapore Statutes Online. The Misuse of Drugs Act.
- 16. Singapore Legal Advice (2019). Singapore’s Drug Laws: Possession, Consumption and Trafficking. https://singaporelegaladvice.com/law-articles/what-are-singapores-laws-on-drug-consumption/
Authors’ Biography Celine Cheow is a fourth year Pharmacy student doing a minor in Forensic Science. She is a member of CJC-F, and is passionate about forensics, especially in the area of illicit drug detection. She hopes to be a forensic toxicologist in the future.
Celine Cheow is a fourth year Pharmacy student doing a minor in Forensic Science. She is a member of CJC-F, and is passionate about forensics, especially in the area of illicit drug detection. She hopes to be a forensic toxicologist in the future. Muhammad Khairul Fikri is a Year 3 undergraduate from the Faculty of Arts and Social Sciences. Khai is one of the Project Managers of “Drugs & Forensics”. He is pursuing a Major in Geography and two Minors; Forensic Science and Geographical Information Systems. He is interested in the applications of technology, particularly geospatial technologies, in forensic science and crime scene investigations.
Muhammad Khairul Fikri is a Year 3 undergraduate from the Faculty of Arts and Social Sciences. Khai is one of the Project Managers of “Drugs & Forensics”. He is pursuing a Major in Geography and two Minors; Forensic Science and Geographical Information Systems. He is interested in the applications of technology, particularly geospatial technologies, in forensic science and crime scene investigations.







